Content deleted Content added
|
|
Line 37:
==Causes==
Unconjugated hyperbilirubinemia during the neonatal period describes the history of nearly all individuals who suffer from kernicterus. It is thought that the [[blood–brain barrier]] is not fully functional in neonates and therefore bilirubin is able to cross the barrier. Moreover, neonates have much higher levels of bilirubin in their blood due to 1):
# the rapid breakdown of fetal red blood cells immediately prior to birth (and subsequent replacement by normal adult human red blood cells). This breakdown of fetal red blood cells releases large amounts of bilirubin. Following on from this 2)
# Neonates cannot metabolize and eliminate bilirubin. The sole path for bilirubin elimination is through the uridine diphosphate glucuronosyltransferase isoform 1A1 (UGT1A1) proteins that perform a (SN2 conjugation) reaction called "glucuronidation". This reaction adds a large sugar to the bilirubin and makes it more water soluble, so more readily excreted via the urine and/or the faeces. The UGT1A1 enzymes are present, but not active until several months after birth in the newborn liver (Miyagi and Collier 2011). Apparently, this is a developmental compromise since the maternal liver and placenta (Collier et al. 2002a, Collier et al. 2002b) perform glucuronidation for the fetus. In the early 1980s a late-fetal change (30 – 40 weeks of gestation) in hepatic UGT1A1 (from 0.1% to 1.0% of adult activity levels) and post-natal changes that are related to birth age not gestational age were reported (Kawade & Onishi 1981). Despite these activity differences, similar levels of protein expression were observed between a 13-week neonate and an adult liver and Burchell et al. (1989) demonstrated UGT maturation with fetal and neonatal liver samples from several gestational time points. Similar development of activities to pan-specific substrates were observed except for serotonin (1A4), where adult activities were observed in fetal (16 – 25 weeks) and neonatal liver up to 10 days old (Burchell et al. 1989). More recently, individual UGT isoform development in infants and young children, including two fetal liver samples, were analyzed and showed that pediatric levels of mRNA and protein for UGT1A1 did not differ from adults, but activities were lower (Strassburg et al. 2002). Hence, the effects of UGT1A1 developmental delay in activation have been illuminated over the last 20–30 years. The molecular mechanism(s) for activating UGT1A1 remain unknown.
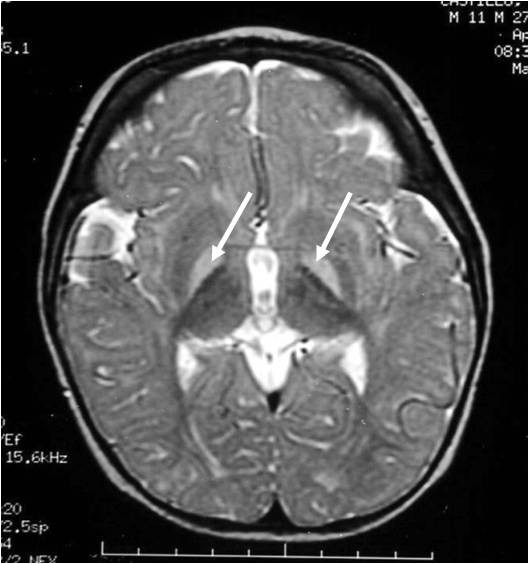
Bilirubin is known to accumulate in the gray matter of neurological tissue where it exerts direct neurotoxic effects. It appears that its neurotoxicity is due to mass-destruction of neurons by apoptosis and necrosis.
|
 Article Images
Article Images